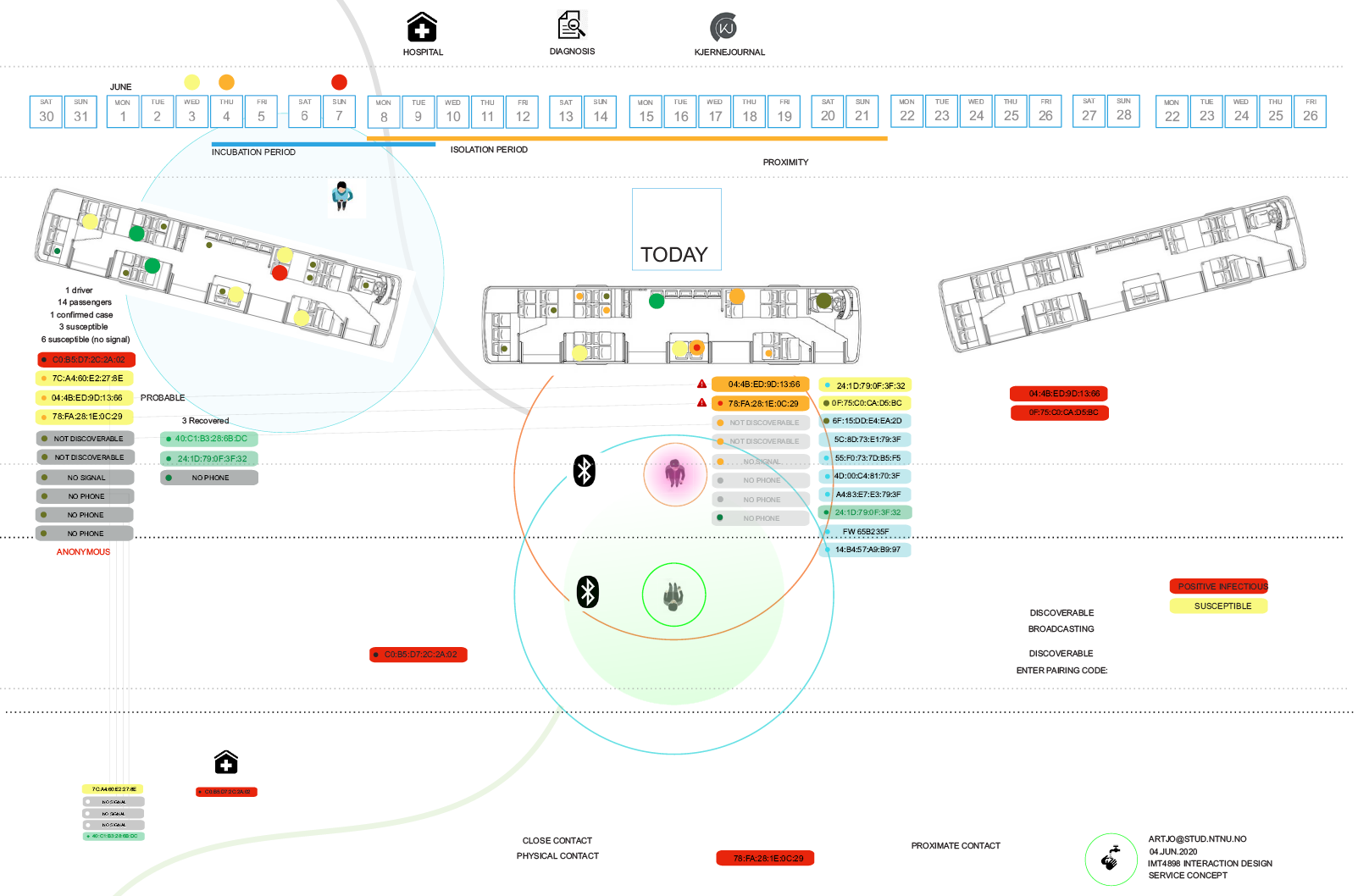
Bus transit nodes and public interchanges adopt routines for curbing Covid-19
In response to the coronavirus pandemic, ambitious startup programs developing and beta-testing proximal and near-network contact-tracing apps utilizing Bluetooth (LE) technology to combat COVID-19 met a backlash in consumer response with the rejection of the social navigation apps using centralized data collection models in the collection of (RSS) signal, device ID information, and the tracking of user activity through GPS coordinates.
The ambitious early goals for national program adoption rates o 60%-80% cited for the NHS program and the Norwegian Folkehelseinstituttet’s app, Smittestopp (FHI) may have set higher benchmarks than necessary to achieve a measurable impact on transmission rates (Kelion, 2020). Simulations built on micro-scale situational populations demonstrate that public-health interventions can be evaluated for efficacy at transit nodes or civic locales (NTB,2020).
Many prototypes have been presented based on a centralized data collection model, but most programs have adopted a user-centered or mesh data collection architecture based on the Google-Apple (GAEN API). Device-independent data collection, built on a premise of user-centered data architecture, shares proximity data about exposure and exposure risk (susceptibility) incidents in an anonymized notification or via the national health authority. Some of the contested architectures transfer user data to server-centered administration plans.
While the public is largely supportive of public health emergency efforts, there is a critical balance between individual rights for privacy, autonomy, and confidentiality and the greater public good. Interventional actions, use, and access to patient records and client data are justifiable based on informed consent (signed-release) and verified risk of public exposure to infectious contagions. Quality control (QC) and quality assurance (QA) standards for determining these civic epidemiological definitions and the bodies responsible for them need to be publicly accountable.
Mission drift, misuse, or inconsistent use of data from one community stakeholder to the next can damage program goals or cause unneeded liabilities and conflicts of interest that undermine the primary purposes of a contact tracing program.
Device capabilities and signal characteristics are one level of the problem. Single device Bluetooth low-energy (BLE) signal accuracy is inconsistent between device types, and environmental obstructions can affect signal and positioning accuracy. Multi-point sensors or multi-device data aggregation could improve the location and distance accuracy but necessarily presents data sharing protocols between hosts. Also, device range and proximity capabilities need to be calibrated to the social-distancing profiles that define exposure incidents and risk. The health authorities usually establish these, and National standards vary considerably from country to country on metrics of social distancing, exposure duration, and the use of patient health records and personal data. Meanwhile, the apps of various manufacturers enable settings to be freely customized.
The result is a field of poorly standardized products. Some are not much more than haptic vibrators and bleeping noisemakers. The effectiveness of simple signal reception and alerts to produce a “user experience” cannot be counted as a consistent measure of exposure or risk.
Public health authority recommendations are issued for social distance independent from individual patient data, introducing yet another level of detail and specificity about personal health status. The SEIR epidemiological compartments are the next level of population-status data with their attending criteria. SEIR represents the most widely recognized prioritized standard variables for epidemiological simulation.
The issue of user participation and adoption rates underscore the importance of standardized and prioritized metrics and statistical models to serve best the contact tracing goals and a social navigation technology that suits participant privacy concerns. (McMurry & Kreps, 2020)